When people search for Adaptog, they usually want to know: Is this a credible health science company, what do they do, and how do their products compare to today’s weight-loss medicines like semaglutide, tirzepatide, and investigational retatrutide?
Adaptog positions itself as a health-science and metabolic wellness company. Their mission is to help people tackle weight-related diseases through medicines, technology, and clinician support. On their website, they highlight bold goals impacting 2.5 billion people by the end of the decade while offering access to modern GLP-1 based therapies.
But to really answer who Adaptog are, you need context: the medicines they are connected to, what those medicines do, and how much evidence backs them up.
Adaptog’s Space: GLP-1 and Beyond
Adaptog operates in the same high-growth space as today’s GLP-1 receptor agonists and newer multi-agonists. These medicines semaglutide, tirzepatide, and the in-trial retatrutide are reshaping weight-management care. Adaptog markets itself as a bridge between these scientific breakthroughs and the people who might benefit from them, with products developed by healthcare professionals.
What These Medicines Are?
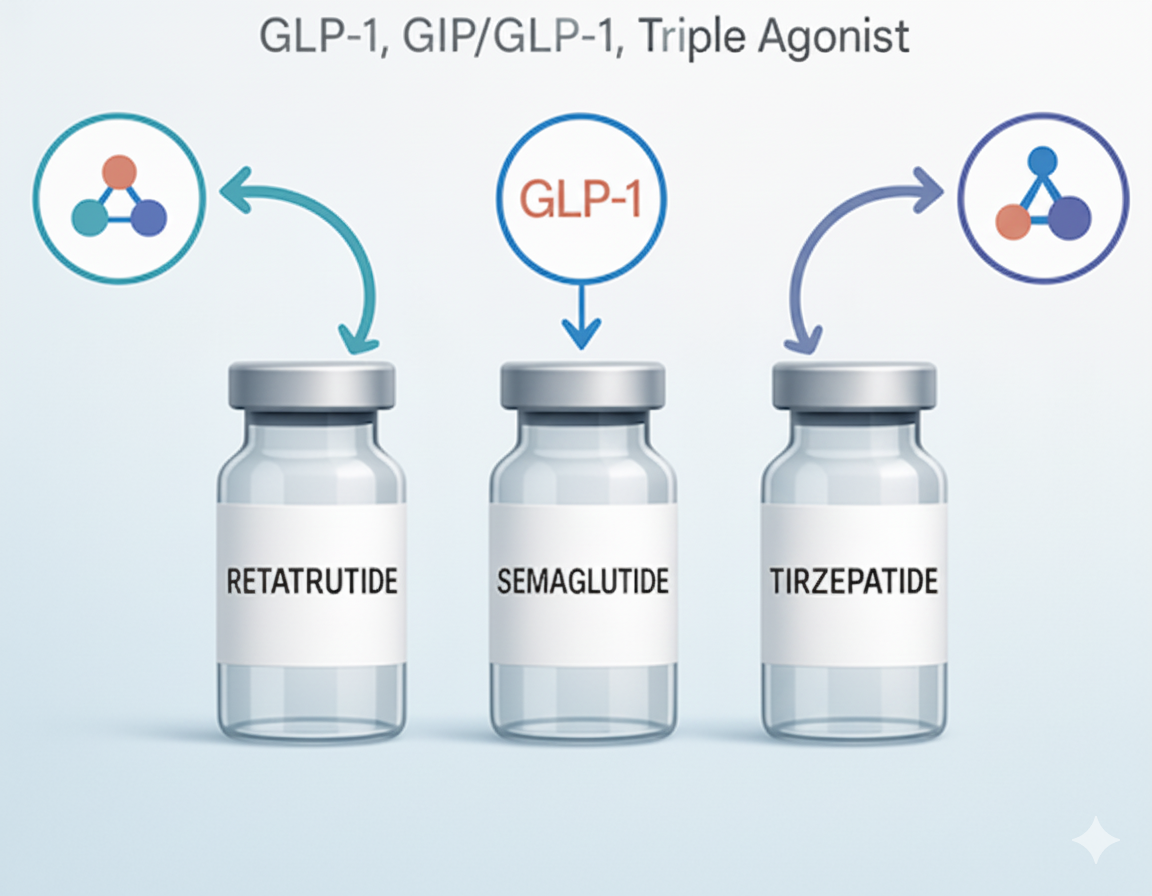
- Semaglutide GLP-1 receptor agonist treats type 2 diabetes and chronic weight. Lifestyle adjustments and semaglutide helped participants lose more weight than placebo in a 68-week experiment.
- Tirzepatide activates GIP and GLP-1 receptors. The 72-week tirzepatide experiment showed significant and sustained weight loss in obese adults.
- Retatrutide is an investigational “triple agonist” that targets GIP, GLP-1, and glucagon receptors. In a 48-week phase 2 study, retatrutide produced substantial weight loss. It is not yet approved.
How Do They Work?
Think of these as “signals” that help your body manage appetite and glucose.
- Semaglutide sends one signal (GLP-1).
- Tirzepatide sends two signals (GIP + GLP-1).
- Retatrutide sends three (GIP + GLP-1 + glucagon).
More signals are not always better for every person, yet comparing retatrutide vs tirzepatide shows how different receptor targets can shape average weight loss and side-effect patterns.
What People Often Notice in Real Life
- Less “food noise” and fewer cravings once semaglutide or tirzepatide reaches a steady dose.
- Earlier fullness at meals and smaller portions on semaglutide or tirzepatide.
- With retatrutide in trials, strong weight-loss signals during titration, with the caveat that more study is needed before approvals.
Pocket Profiles (Use with Clinical Advice)
Semaglutide
- Best for: People wanting a single-path GLP-1 alternative with solid long-term obesity data and a dedicated cardiovascular outcomes trial in overweight/obese people with existing cardiovascular disease.
- What People notice: A weekly regimen, gradual hunger control, and weight loss over months.
- How to use: Keep a simple diet and exercise regimen and take a weekly injection with moderate dose increases to reduce GI problems.
- First to pause/ask: People with GI problems, pancreatitis, or medullary thyroid cancer should address hazards. Consult product labels and your doctor.
Tirzepatide
- Best for: Adults who may benefit from dual-path signaling (GIP + GLP-1) and larger average weight loss in trials.
- What people notice: Strong appetite suppression and notable weight change with continued use and lifestyle support.
- How to use: Weekly injection with stepwise titration; consistent follow-up for dose and side-effect management.
- Who should pause/ask first: Same thyroid and pancreatitis caution apply; review drug interactions and pregnancy plan with a clinician.
Retatrutide

- Best for: Research settings at this stage; retatrutide is investigational and not yet approved. Early trials report meaningful retatrutide benefits, including large average weight reductions by week 48 in phase 2, with phase 3 needed to confirm outcomes.
- What people notice: In trials, strong weight-loss signals at higher doses; real-world access awaits phase 3 results and regulatory review.
- How to use: Use is only within clinical studies right now, where retatrutide dosing for weight loss follows a set protocol for timing, dose, and monitoring.
- Who should pause/ask first: Anyone outside a study, because it is not approved. More safety and outcomes data are in progress.
The 4-S Method to Choose with Your Clinician
- Status: List your current diagnoses, meds, and goals in one page.
- Signals: Discuss whether single (GLP-1), dual (GIP + GLP-1), or triple signaling fits your risk profile and targets.
- Side effects: Plan for GI effects and create a food, hydration, and dose-timing routine to reduce them.
- Sustain: Agree on monitoring, activity goals, and how to handle plateaus without abrupt stops.
What the Strongest Studies Say?
- In STEP-1, semaglutide 2.4 mg for 68 weeks led to clinically relevant weight loss versus placebo alongside lifestyle changes.
- In SURMOUNT-1, tirzepatide for 72 weeks produced substantial and sustained weight reductions in adults with obesity.
- In a large cardiovascular outcomes trial (SELECT), semaglutide reduced major cardiovascular events in adults with overweight/obesity and established cardiovascular disease.
- In a 48-week phase 2 study, retatrutide showed large mean weight losses; approvals require successful phase 3 results.
Dosing, Timing, and What Actually Matters
Dose increases are slow by design; if you are in a study, confirm your assigned retatrutide dose and the step-up schedule that fits the protocol. That pacing helps your body adapt and can reduce nausea. Build a simple weekly routine for injections, a gentle meal structure with adequate protein and fiber, and daily movement that you can keep doing. Keep a short log and share it at check-ins.
What to track
- Weekly weight trend and waist measure
- Meal size, fullness, and any nausea
- Activity minutes and sleep quality
When This Is the Wrong Tool
- If you’re pregnant, planning pregnancy, or breastfeeding
- If you have active, significant GI disease or prior pancreatitis
- If you or close family have MTC or MEN2 (talk to your clinician)
- If you cannot commit to regular monitoring and dose adjustments
Safety, Interactions, Side Effects
- Common effects include nausea, vomiting, diarrhea, and constipation during titration; slow dose steps and simple meals help.
- Discuss other diabetes medicines to avoid low blood sugar when combined, and ask specifically about tirzepatide and alcohol so you understand safe limits and timing.
- Report severe or persistent abdominal pain, dehydration, or signs of gallbladder issues promptly.
FAQs
Which works best on average: retatrutide vs semaglutide vs tirzepatide?
Trials show strong weight loss with semaglutide and very strong results with tirzepatide over 68–72 weeks. Retatrutide has shown large losses in a 48-week phase 2 study, yet it remains investigational until phase 3 confirms benefits and safety. Individual results vary and depend on dose, adherence, and support plans.
Is retatrutide available now?
Not yet. Retatrutide is in clinical development. Phase 2 data are published, and larger phase 3 studies are underway or planned. Approval decisions will follow those results.
Does semaglutide have heart benefits beyond weight loss?
In adults with overweight/obesity and established cardiovascular disease, semaglutide reduced major adverse cardiovascular events versus placebo. This supports discussions about risk reduction with your cardiometabolic team.
How is tirzepatide different from semaglutide in day-to-day use?
Tirzepatide targets two receptors instead of one, and trials show larger average weight loss at approved doses. Both are weekly injections with slow titration, similar GI effects, and the same safety warnings about thyroid cancer history and pancreatitis. Your clinician will match dose and pacing to your profile.
Research About GLP-1, GIP, and Triple-Agonist Medicines
- Concept & caution: These medicines act on metabolic signaling rather than “boosting willpower.” Benefits are real but require steady routines and careful titration; labels carry pregnancy and thyroid warnings, so keep claims modest and decisions clinician-led.
- Mechanisms & appetite/glucose networks: Reviews and trials describe GLP-1 (± GIP) signaling that slows gastric emptying, curbs appetite, and improves glycaemic control; triple-agonists add glucagon-pathway effects that may enhance energy expenditure in trials.
- Tirzepatide & sustained weight control: A 72-week study reported substantial weight loss, with long-term analyses suggesting limited gain for many participants under continued care.
- Semaglutide & cardiovascular outcomes: In adults with overweight/obesity and established CVD, semaglutide reduced major adverse cardiovascular events versus placebo.
- Retatrutide (triple agonist): Phase 2 data showed large average weight reductions by 48 weeks; phase 3 and regulatory decisions are pending, so real-world use awaits further evidence.
Final Thoughts
Honestly, these medicines aren’t magic. They don’t replace the basics. Think of semaglutide, tirzepatide, and retatrutide as quiet helpers that make consistent choices easier, less grazing, calmer portions, steadier weeks. They work best when you keep the foundation simple: regular meals with enough protein, daily movement you can repeat, real sleep, and regular follow-ups.
Start low, go slow, notice how you feel, and keep your clinician in the loop. No hype. Just steady, supported change. Ready to explore semaglutide, tirzepatide, and other trusted compounds with confidence? Visit UK Peptides today and discover research-grade quality backed by UK reliability.
References
- Jastreboff, Ania M., Lee M. Kaplan, Juan P. Frías, Qiwei Wu, Yu Du, Sirel Gurbuz, Tamer Coskun, Axel Haupt, Zvonko Milicevic, and Mark L. Hartman. “Triple–hormone-receptor agonist retatrutide for obesity—a phase 2 trial.” New England Journal of Medicine 389, no. 6 (2023): 514-526.
- Wilding, John PH, Rachel L. Batterham, Salvatore Calanna, Melanie Davies, Luc F. Van Gaal, Ildiko Lingvay, Barbara M. McGowan et al. “Once-weekly semaglutide in adults with overweight or obesity.” New England Journal of Medicine 384, no. 11 (2021): 989-1002.
- Jastreboff, Ania M., Louis J. Aronne, Nadia N. Ahmad, Sean Wharton, Lisa Connery, Breno Alves, Arihiro Kiyosue et al. “Tirzepatide once weekly for the treatment of obesity.” New England Journal of Medicine 387, no. 3 (2022): 205-216.
- Lincoff, A. Michael, Kirstine Brown-Frandsen, Helen M. Colhoun, John Deanfield, Scott S. Emerson, Sille Esbjerg, Søren Hardt-Lindberg et al. “Semaglutide and cardiovascular outcomes in obesity without diabetes.” New England Journal of Medicine 389, no. 24 (2023): 2221-2232.
- Windram M, Lovelock DF, Carew JM, Krieman CG, Hendershot CS, Besheer J. Semaglutide, tirzepatide, and retatrutide attenuate the interoceptive effects of alcohol in male and female rats. Psychopharmacology (Berl). 2025 Jul 23. doi: 10.1007/s00213-025-06854-3. Epub ahead of print. PMID: 40699363.
FDA. Wegovy (semaglutide) Prescribing Information—warnings, dosing, population guidance. Updated 2024. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/215256s011lbl.pdf